|
| As a SuppVersity reader you know that training at high altitudes can burn tons of fat and build muscle in competitive swim- mers, but is the corresponding study more than just the literal exception to the rule? |
In an ahead of print review of the literature on hypoxic training in the
Journal of Science and Medicine in Sport researchers from the
Department of Physiotherapy at the
Tan Tock Seng Hospital in Singapore and the
Bond Institute of Health & Sport at the
Faculty of Health Science and Medicine of the
Bond University in Australia present some pretty intriguing health benefits of training in low oxygen environments (hypoxia = "low oxygen").
Since I am well aware of the fact that "health" is not exactly as sexy as the improvements in lean mass increases, Bailey et al. report in a paper from the year 2000, or the body fat reductions Greie et al. report in their 2006 paper on training in low exercise environments.
I decided to expand what was originally intended as a(n already) longer note in the
SuppVersity Facebook News into my own review of the literature; a review that would embrace both, the beneficial health effects and the improvements in body composition and exercise performance of which I know that they are what many of you are most interested in.
Hypoxic training vs. blood flow restriction - two fundamentally different things: As a faithful
SuppVersity reader this is not the first time you've read about hypoxia training, here at the
SuppVersity (
browse the
SuppVersity Archives). In view of the fact that people regularly confuse hypoxia training, which happens either in naturally "thin air" at high altitudes or in special chambers and tents that are filled with air with subnormal oxygen content, with blood flow restricted (BFR) / Katsu training, I still want to make sure that we are not talking about blood flow restriction, here (you can learn more about that➲
here).
I initially thought, it may be best to simply tackle study by study, but then decided that the article would become to long and the information to difficult to grasp. That's why I have structured the following overview of the contemporarily available evidence based on the effects and stuck to the outcome for most of the cited studies. If you want to learn more, you can always follow up on the references at the bottom of the page; but you know that, anyways - dont' you?
- Muscle structure / characteristics: There is little specific
research that deals with the muscle tissue adaptations to hypoxic
training, but in an excellent review of the little evidence we have from
study with other endpoints, Hoppler and Vogt emphasize the following adaptive changes in muscle structure, enzyme expression & co:
 |
| Figure 1: Even the fiber composition changes in response to 4 weeks low resis- tance / high leg training in hypoxia vs. normoxia (Friedmann. 2003) |
initial
decrease in muscle oxidative capacity which provides a stimulus for
compensation and subsequent increases in exercise performance at see
level- upregulation of the regulatory subunit of hypoxia-inducible factor-1 (HIF-1)
- increase in myoglobin, endothelial growth factor and glycolytic enzyme mRNA expression
- increases in mitochondrial and capillary densities
Basically
these changes are at the heart of both the performance increases
discussed in the next paragraph, as well as many of the health benefits
we will analyze at the end of this article.
What is hypoxic training? "Hypoxic training, commonly referred to as altitude training, refers to the use of normobaric or hypobaric hypoxia (reduced oxygen concentration, <20.93%), in an attempt to emulate altitude acclimatization to attain improved athletic performance. Normobaric hypoxic training incorporates the use of masks and chambers, whereas hypobaric hypoxic training involves ascending to elevated environments. Hypoxic training can be conducted in normobaric or hypobaric conditions with the use of masks, chambers or by ascending to elevated environments (Wee. 2013)
Performance effects: Actually the increase in athletic performance was the original purpose of high altitude training camps, which became increasingly popular in the aftermath of the 1968 Mexico City Olympics Games (held at an altitude of
2300 m), where athletes, coaches and "experts" were surprised by the poor results that were observed in endurance events. It is thus no wonder that this is one of the best researched, albeit not most exciting applications of hyperbaric and normobaric [explanation see box to the right] hypoxic training.
As Levine et al. point out in their 2005 paper on the positive effects of intermittent hypoxia (live high: train low) on exercise performance, these effects are mediated primarily, but not exclusively, by augmented red cell volume (Levine. 2005) - natural erythripoetin (EPO), if you will. It is thus no wonder that these effects won't occur if you get into a hypobaric environment for less than 70min 5x per week (cf. Julian 2004), but require chronic exposure, i.e. during exercise and rest as it would be the case in one of the many altitude training athletes can chose from.
 |
| The benefits of intermittent HT (90min 3x/week for 3 weeks) are negligible (Katayama. 2003) |
Adaptation requires chronic exposure to a low oxygen environment: Studies on short-term hypobaric (training + living at high altitude) and intermittent normobaric training
(training in a tent or with a mask) have yielded very mixed results. This is why Wilber et al. recommend in a 2007 overview article in
Medicine And Science In Sports And Exercise that athletes who want to gain performance benefits from hypoxic training "need to live at a natural elevation of 2000-2500 m for > or=4 wk for > or=22 h/day" (Wilber. 2007).
Millet et al. add in an article in
Sports Medicine from 2010 that hopoxic training is one of the few cases where "[l]onger is better as regards haematological changes". Hypoxic exposures of less than 12h/day are simply insufficient to trigger an increase in erythropoiesis. The researchers do yet also point out that "[f]or non-haematological changes, the implementation of a much shorter duration of exposure does seems possible" (Millet. 2010).
- With intermittent hypoxia training these conditions are not met and the results are either disappointing or, as in Roels et al. 2007, who found that "[i]ntermittent training performed in hypoxia was less efficient for improving endurance performance at sea level than similar training performed in normoxia" (Roels. 2007) downright detrimental. When it's done "right", on the other hand, even professional athletes can expect substantial enhancement of maximal endurance power output natural "live-high-train-low" regimen of ca. 4% (Bonetti. 2009; meta-analysis of 51 studies).
As Bonetti et al. elaborate in their 2009 meta-analysis of data from 51 controlled trials, the type of training had a major impact on the effects in subelite athlete who achieved performance increases of 3.5-6.8% even with intermediate hypoxia training. In elite athletes the performance increase in live-high-train-high and live-high-train-low scenarios were 5.2% and 4.3% respectively. The researchers also conclude that the endurance power VO2 max increased in subelite athletes, only. In elite athletes, on the other hand, there was a tendency for (termporary) reductions in VO2 (see figure in "adaptation requires chronic exposure" box) for Bonetti et al. cannot explain.
-
Increases in muscle size: "Yes!" That's the answer to what is in their eyes the most important question people ask me, whenever I talk about alternative training regimen. Yes, it will help you gain muscle. Due to the scarcity of evidence, it is yet difficult to say, whether it's going to help you to gain more muscle than on a regular hypertrophy regimen.
What I can tell you though, is that even studies that were intended to measure the effects on metabolic and cardiovascular risk factors in men report significant increases in lean muscle mass (Bailey. 2000). What's particularly impressive about this study is the fact that the 18 subjects who had been randomly assigned to the hypoxic training group gained lean mass (+2%), while those 14 subjects who did their 20 –30 min of cycling at 70 – 85% of their individual maximal heart rates under normoxic lost a minimal amount of lean mass.
 |
| Figure 2: Changes in triceps and biceps cross sectional area after 18 biceps workouts in hypoxic or normoxic environment; %-ages over the bars indicate rel. pre-post change (Nishimura. 2010) |
In a more strength training specific study from 2010 Nishimura et al. report similarly more pronounced increases in sleeve sizes in those of their 14 male university students who had been randomized to perform their 4 sets of biceps curls and triceps extensions at 70% of their individual 1-RM max in a hypoxic environment. After 6 weeks and 18 workouts (three workouts per week), the scientists from the Mie University Graduate School of Medicine in Japan found that the 7 participants in the hypoxic training group had experienced significantly greater biceps and triceps hypertrophy, than their peers in the control group (Nishimura. 2010; see Figure 2).
Think of hypoxic training as an intensity technique: If you think of hypoxic training as an intensity technique that provides you with an additional stressor. It should be obvious that advanced trainees should benefit more than rookies from a 1:1 comparison such as the one Nishimura et al. conducted. For the rookie the regular exercise stimulus is enough (sometimes even too much) to grow, for the advance athletes the ever-same 3x10-regimen gets kicked up a notch, when he/she trains in a hypoxic environment, because the lack of oxygen will provide famous "+1" in the "i+1" principle of skeletal muscle hypertrophy that can easily get lost after months and years of training.
- Needless to say that it would be great if we had more scientific evidence from actual resistance training studies such as the one by Nishimura - I mean, the results they present look pretty fascinating - specifically in view of the fact that we are neither dealing with the kind of pussy training that's applied in the average blood flow restriction study (high reps, low weight; latest example: 30 reps at 30% 1 RM, learn more), nor subjects for whom the walk from the couch to the fridge is already a challenge.
- Metabolism & fat loss: Now that we have discussed the #3 and #2 on the SuppVersity top-list of most requested topics, we get to the #1 on the list: The metabolic effects of training in hypoxia and its ability to instigate fat loss. I've mentioned one of them, i.e. the study by Greie et al. (2006) in the introduction, already. In view of the fact that their main interest was in the improvement of metabolic syndrome markers that could be achieved in the course of a three week altitude specific hiking vacation", it's only logical that the 71 volunteers (age 36-66 yr old) who participated in the study were obese and exhibited all the metabolic abnormalities, the of the WHO definition of MetSyn (WHO. 1999).
An additional word of caution: Unless you actually work out, the
constant stress you're exposed to when living in a hypoxic environment
will cause muscle atro- phy. This is a well- established fact (Surks. 1966)
and a serious problem for mountaineers (Boyer. 1984), who aren't
accustomed to the low oxygen content in high altitudes. An example would
be the 5.9kg weight loss in Caucasian participants of American Medical
Research Expedition to Everest in 1981. Luckily, 70.5% of the weight
most of which >75%, was lost not during the ascend, but during the
residence above 5,400 m was fat (Boyer. 1984). Interes- tingly, the
Sherpas, who arrived in Base Camp with half as much body fat as members
(9.1% vs. 18.4%), maintained weight and limb circumferences during
residence above 5,400 m - adaptation, I'd guess.
Whether or not the metabolic improvements the subjects achieved in the 29h of light exercise, that included 12 moderate- intensity guided hiking tours (4 times/week, 55-65% HRmax) and individual "moderate recreational activities" would be observed in lean individuals would thus still have to be confirmed. That doesn't change the fact, though, that the significant and lasting (at least for 1 week after the subjects returned) decreases fasting insulin and homeostasis model assessment (HOMA)-index, was a prerogative of those subjects who had been randomized to the moderate altitude group (1,700m).
 |
| Figure 3: Rel. changes (%) of BMI, lean and fat mass in Chinese Swimmers during 3 weeks in normal (control) and high altitude (altitude) training camp (Chia. 2013) |
As a SuppVersity reader you will also remember that a group of Chinese swimmers achieved even more impressive changes in their physique, i.e. -11% reduction in body fat in the absence of any dietary restriction, within only three weeks in a high altitude training camp (see Figure 3 and read up on the details in ⤹"Shed 11% of Your Total Fat Mass in 3 Weeks: Altitude Training Melts Fat & Builds Muscle in Elite Swimmers" | read more).
Part of the effects we see in studies where the subjects reside in 24h hypoxia in high altitude scenarios may be mediated by either malobsorption, increased expression of thyroid hormones, or a modulatory effect on the satiety hormones and a subsequent reduction in appetite:
- Nutrient malabsorption - Boyer et al. (1984), for example, observed a 48.5% reduction in fat absorption in three of the member of the American Medical Research Expedition to Everest in 1981,
and 6 out of 7 members of the expedition team had a lowered xylose
excretion (24.3%), which is indicative of a reduced sugar absorption.
 |
| Figure 4: Change in thyroid hormone levels in 18 subjects who usually live at sea level after exposure to simulated altitude (3,500m; 4h/d) in a hypoxic chamber for six days (Sawhney. 1991) |
Maxed out thyroid function - The changes in T3 and T4 levels Sawhney et al. observed 1991 in healthy euthyroid sea level residents who were exposed to a simulated altitude of 3500 m in a hypobaric chamber for only 4h on six subsequent days (see Figure 4) were so drastic that you have to wonder that Maswon et al. (2000) report that the energy expenditure of the female participants of their sea level vs. altitude (4,000m) experiment experienced an increase in energy expenditure of "only" 6% (160 kcal/day; Mawson. 2000). - Reduced appetite - Wasse et al. (2011) report reductions in acylated ghrelin (-18%) and increases in the satiety hormone PYY (+7%) in response to 7h in a hypoxic environment. Contrary to the chronic exposure in high altitude camps, of which Westerp-Plantenga et al. report in a 1999 paper that it leads a reduction in energy intake of more than 1,000kcal/per day at altitudes of 5,000-6,000m, well before any symptoms of mountain sickness occur (Westerp-Plantenga. 1999), the acute short term exposure and the corresponding changes in hunger (ghrelin) and satiety (PYY) hormones in the Wasse study didn't have any effects on the actual energy intake of the study participants.
If we compare the results of Wasse and Westerterp-Plantenga (1999) it seems reasonable to assume that the intermediate exposure to normobaric hypoxic environments (just a reminder: that's exercise in a champer or tent that simulates high altitude) wouldn't have any measurable effects on body composition.
 |
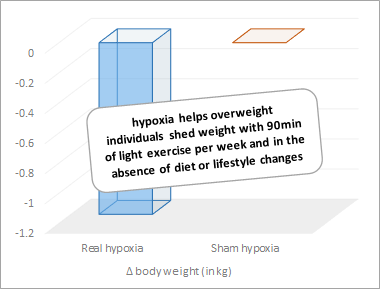
| Figure 5: Changes in body weight during the 8-week exercise only intervention in the Netzer study (Netzer. 2008) |
The results Netzer, Chytra & Küpper present in a 2008 paper do yet disprove the hypothesis that training in a special gym or other low oxygen environment affect the weight loss efforts of the average German 47.6 year-old overweight man or women. A brief glance at the figure to right (Figure 5) does after all suffice to see that the hypoxia group lost 1.14kg of body weight over the course of the 8-week exercise-only (=no energy deficit, lifestyle change, etc.) intervention with thrice weekly 90min sessions of light exercise, while the subjects who had been randomized to the normobaric training group didn't lose a single pound.
In the absence of detailed information about the changes in lean- vs. fat mass and without data on the overall energy intake of the subjects, we are however unable to tell whether the subjects lost only fat and whether the differences were the result of a hypoxia induced reduction in appetite. What we do know, however is that the effects on body weight in intermittent hypoxia training are not the result of a mere placebo effect. The subjects in the "sham hypoxia" (=control) group were after all told they were also training in a low oxygen environment.
- Health benefits: Less sexy, but unquestionably significantly more important than the previously discussed effects on performance and body composition are the effects hypoxia can have on crucial health parameters, such as vascular function, glucose and lipid metabolism and systemic inflammation in both sick and healthy individuals.
At least with respect to the improvements in glucose metabolism, a recent (if not the most recent) that published in the open access journal PLoS|One on August 01, 2013 (Stöwhas. 2013) does yet appear to suggest something different. As expected the lipid profile and systemic
inflammation levels of Stöwhas et al.'s 51 healthy male subjects (mean age of 26.9y) did improve significantly when they were moved from 490m above ground (Zurich) to an altitude of 2590m (Davos) for two days:
 |
| Suggested read: "100-200ml Red Wine Per Day Improve HDL and the LDL/HDL Ratio" | more |
0.14mmol/l reduction in triglycerides (p = 0.012), - 0.08 mmol/l increase in HDL (p<0.001),
- 0.25 reduction in total cholesterol / HDL ratio (p = 0.001),
- 0.45nm increase in average LDL particle size (p = 0.048) and
- 0.18mg/dl reduction in hsCRP (p = 0.024)
Their insulin and glucose levels, on the other hand, remained essentially unchanged. That's not necessarily a bad thing, with glucose and insulin levels of 5.2mmol/L (reduced to 5.1mmol/L during their stay in at 2590m) and 2.0µU/ml, the study participants were after all already way below the cut off limit of the "normal" zone for glucose (< 6.2 mmol/L) and insulin (<10µU/ml). In addition to that, we've got evidence of
- reduced blood pressure in response to a single ~2h hike in normo- and hypertensive individuals (Auer. 2004),
- blood pressure and blood lipid reductions in hypertensive individuals in the previously mentioned trial by Bailey et al. (2000) and a 2001 follow up (Bailey. 2001),
- reductions in triglycerides, fasting insulin and improvements in glucose tolerance in Haufe et al. (15% reduction in oxygen content for 60 min/day, 3 days/week, 4 weeks; 2008),
- improved leptin and glucose metabolism in Kelly (4300 m for only 15 min; 2010), and
- reductions in triglyerides and cholesterol in Minvaleev et al. (2000 m–3000 m for 10 days; 2011) and Wagner et al. (60 min/day, 3 days/week, 4 weeks; 2010).
What's somewhat surprising, though, is that other studies such as Sandoval et al. (13% Duration of 4× incremental exercise test; 2002), Pialoux et al. (10 min mod. exercise 3000m, 3h rest at 4800 m; 2009) and Siqués et al. (3550m for 12 months; 2009) had opposite effect on glucose management, blood lipids and blood pressure in young women, endurance athletes and young adults first exposed to high altitude for 12 months at 3550 m, respectively.
In spite of the relatively scarce and not 100% conclusive evidence, the latest review of the literature does still emphasize the "promising benefits" one can achieve "with the use of moderate levels of hypoxic training in relation to some metabolic risk factors" (Wee. 2013) and point out that hypoxic
training may be used as a treatment option to supplement exercise
training to modulate certain cardiometabolic risk factors although.
I guess, it would be possible to write another 3,000 words about this topic, but by now you should be able to form your own opinion on whether or not it may make sense to spend you next holiday in the Andes or on a trip to the Narga Parbat, the world's ninth highest and one of the most famous mountains in the Himalaya.
 |
| Figure 6:Changes in different mRNAs in vastus lateralis of previously untrained subjects in response to 6 weeks in 4 different groups: nor-high indicates normoxia high intensity; hyp-high, hypoxia high intensity; nor-low, normoxia low intensity; hyp-low, hypoxia low intensity (Vogt. 2010). |
Bottom line: It's honestly difficult to to judge how useful hypoxic training actually is for the average gymrat. For the elite athlete each quantum of additional performance counts and could make the difference between victory and defeat. If you look at the graphical summary Vogt and Hoppeler attached to their 2010 paper (
Figure 6) it does yet appear as if we'd have a similar problem with
intermittent hypoxia training (obviously the only method that's available to the average trainee
- or can you afford to take 6 weeks off and pay for an high altitude training camp?) as with blood flow restriction: There are no real advances over the serious strength training. If you are forced to train at low(er) intensities, though, the additional stressor, hypoxia, could be an ideal means to boost the oxidative capacity of your muscles and increase your fatty acid oxidation and O2 transport.
Similarly prolonged hypoxic exposure is required not only for the beneficial health effects (Wee. 2013), but also for the previously summarized beneficial effects on body composition. If we go by the results of the Nishimura (2011) study, the latter is not the case when we are talking about skeletal muscle hypertrophy - quite logical, actually: I mean, we all know that hypertrophy occurs in response to repeated acute stimuli, anyway.
References:
- Auer, J., Berent, R., Prenninger, M., Weber, T., Kritzinger, K., Veits, M., ... & Eber, B. (2004). Short-Term Effects of a Single Exercise Bout at Moderate Altitude on Blood Pressure. JSR, 13(1).
- Bailey, D. M., Davies, B. & Baker, J. (2000). Training in hypoxia: modulation of metabolic and cardiovascular risk factors in men. Medicine and science in sports and exercise, 32(6), 1058-1066.
- Bailey, D. M., Davies, B., & Young, I. S. (2001). Intermittent hypoxic training: implications for lipid peroxidation induced by acute normoxic exercise in active men. Clinical Science, 101(5), 465-475.
- Boyer, S. J., & Blume, F. D. (1984). Weight loss and changes in body composition at high altitude. Journal of Applied Physiology, 57(5), 1580-1585.
- Chia, M., Liao, C. A., Huang, C. Y., Lee, W. C., Hou, C. W., Yu, S. H., ... & Kuo, C. H. (2013). Reducing Body Fat with Altitude Hypoxia Training in Swimmers: Role of Blood Perfusion to Skeletal Muscles. Chinese Journal of Physiology, 56(1), 18-25.
- Friedmann, B., Kinscherf, R., Borisch, S., Richter, G., Bärtsch, P., & Billeter, R. (2003). Effects of low-resistance/high-repetition strength training in hypoxia on muscle structure and gene expression. Pflügers Archiv, 446(6), 742-751.
- Greie, S., Humpeler, E., Gunga, H. C., Koralewski, E., Klingler, A., Mittermayr, M., ... & Schobersberger, W. (2006). Improvement of metabolic syndrome markers through altitude specific hiking vacations. Journal of endocrinological investigation, 29(6), 497-504.
- Haufe, S., Wiesner, S., Engeli, S., Luft, F. C., & Jordan, J. (2008). Influences of normobaric hypoxia training on metabolic risk markers in human subjects. Med Sci Sports Exerc, 40(11), 1939-1944.
- Katayama, K., Matsuo, H., Ishida, K., Mori, S., & Miyamura, M. (2003). Intermittent hypoxia improves endurance performance and submaximal exercise efficiency. High altitude medicine & biology, 4(3), 291-304.
- Kelly, K. R., Williamson, D. L., Fealy, C. E., Kriz, D. A., Krishnan, R. K., Huang, H., ... & Kirwan, J. P. (2010). Acute altitude-induced hypoxia suppresses plasma glucose and leptin in healthy humans. Metabolism, 59(2), 200-205.
- Levine, B. D., & Stray-Gundersen, J. (2005). Point: positive effects of intermittent hypoxia (live high: train low) on exercise performance are mediated primarily by augmented red cell volume. Journal of applied physiology, 99(5), 2053-2055.
- Mawson, J. T., Braun, B., Rock, P. B., Moore, L. G., Mazzeo, R., & Butterfield, G. E. (2000). Women at altitude: energy requirement at 4,300 m. Journal of Applied Physiology, 88(1), 272-281.
- Millet, G. P., Roels, B., Schmitt, L., Woorons, X., & Richalet, J. P. (2010). Combining hypoxic methods for peak performance. Sports medicine, 40(1), 1-25.
- Minvaleev, R. S. (2011). Comparison of the rates of changes in the lipid spectrum of human blood serum at moderate altitudes. Human Physiology, 37(3), 355-360.
- Netzer, N. C., Chytra, R., & Küpper, T. (2008). Low intense physical exercise in normobaric hypoxia leads to more weight loss in obese people than low intense physical exercise in normobaric sham hypoxia. Sleep and Breathing, 12(2), 129-134.
- Nishimura, A., Sugita, M., Kato, K., Fukuda, A., Sudo, A., & Uchida, A. (2010). Hypoxia increases muscle hypertrophy induced by resistance training. International journal of sports physiology and performance, 5(4), 497.
- Pialoux, V., Mounier, R., Rock, E., Mazur, A., Schmitt, L., Richalet, J. P., ... & Fellmann, N. (2009). Effects of acute hypoxic exposure on prooxidant/antioxidant balance in elite endurance athletes. International journal of sports medicine, 30(02), 87-93.
- Sandoval, D. A., & Matt, K. S. (2002). Gender differences in the endocrine and metabolic responses to hypoxic exercise. Journal of Applied Physiology, 92(2), 504-512.
- Sawhney, R. C., & Malhotra, A. S. (1991). Thyroid function in sojourners and acclimatised low landers at high altitude in man. Hormone and metabolic research, 23(02), 81-84.
- Siqués, P., Brito, J., Banegas, J. R., León-Velarde, F., de la Cruz-Troca, J. J., López, V., ... & Herruzo, R. (2009). Blood pressure responses in young adults first exposed to high altitude for 12 months at 3550 m. High altitude medicine & biology, 10(4), 329-335.
- Stöwhas, A. C., Latshang, T. D., Cascio, C. M. L., Lautwein, S., Stadelmann, K., Tesler, N., ... & Kohler, M. (2013). Effects of acute exposure to moderate altitude on vascular function, metabolism and systemic inflammation. PloS one, 8(8), e70081.
- Surks, M. I., Chinn, K. S., & Matoush, L. R. (1966). Alterations in body composition in man after acute exposure to high altitude. Journal of applied physiology, 21(6), 1741-1746.
- Ventura, N., Hoppeler, H., Seiler, R., Binggeli, A., Mullis, P., & Vogt, M. (2003). The response of trained athletes to six weeks of endurance training in hypoxia or normoxia. International journal of sports medicine, 24(03), 166-172.
- Vogt, M., Puntschart, A., Geiser, J., Zuleger, C., Billeter, R., & Hoppeler, H. (2001). Molecular adaptations in human skeletal muscle to endurance training under simulated hypoxic conditions. Journal of Applied Physiology, 91(1), 173-182.
- Vogt, M., & Hoppeler, H. (2010). Is hypoxia training good for muscles and exercise performance?. Progress in cardiovascular diseases, 52(6), 525-533.
- Wagner, P. D., Sutton, J. R., Reeves, J. T., Cymerman, A., Groves, B. M., & Malconian, M. K. (1987). Operation Everest II: pulmonary gas exchange during a simulated ascent of Mt. Everest. Journal of Applied Physiology, 63(6), 2348-2359.
- Wasse, L. K., Sunderland, C., King, J. A., Batterham, R. L., & Stensel, D. J. (2012). Influence of rest and exercise at a simulated altitude of 4,000 m on appetite, energy intake, and plasma concentrations of acylated ghrelin and peptide YY. Journal of Applied Physiology, 112(4), 552-559.
- Wee, J., & Climstein, M. (2013). Hypoxic training: Clinical benefits on cardiometabolic risk factors. Journal of Science and Medicine in Sport.
- Westerterp-Plantenga, M. S., Westerterp, K. R., Rubbens, M., Verwegen, C. R., Richelet, J. P., & Gardette, B. (1999). Appetite at “high altitude”[Operation Everest III (Comex-’97)]: a simulated ascent of Mount Everest. Journal of Applied Physiology, 87(1), 391-399.
- WHO, Consulation (1999). Definition, diagnosis and classification of diabetes mellitus and its complications. Geneva, Switzerland: World Health Organization, 31(3), 1-59.
- Wilber, R. L., Stray-Gundersen, J., & Levine, B. D. (2007). Effect of hypoxic" dose" on physiological responses and sea-level performance. Medicine and science in sports and exercise, 39(9), 1590-1599.